Human-in-the-Loop (HITL). It’s inside every AI pitch deck and RFP response that crosses an IT leader’s desk. The words sound rigorous, implying that someone is always watching to make sure that an AI model acts responsibly.
But here are two questions worth asking: Who is the appropriate human to keep in the loop, and exactly where in the process should they sit? The answers matter, especially in the context of scheduling, where inaccurate AI outputs missed by humans can mean the difference between health system growth and optimizing your clinical capacity, or a bad experience where patients can’t access the care they need.
Two Models. One Big Difference.
There are two different ways to incorporate a human-in-the-loop into an AI-enabled scheduling system.
In the first model, generative AI (GenAI) searches across all available data and produces a response. A patient access team member reviews the output and, if anything looks wrong, corrects it.
The problem with this approach is that human reviewers have limited visibility into where the AI found its data or how it generated a response. If the underlying data is wrong, GenAI can produce a confident-sounding—but erroneous—answer, which a human reviewer may not identify. GenAI also can’t find data that doesn’t live in any system, and in specialty scheduling, most booking rules live in people’s heads, not in a file.
In the second model, humans come first. Schedulers and other patient access staff who own the knowledge review, approve, and lock the data before AI uses it to answer booking or patient routing questions. AI never makes the final call. Instead, it retrieves data from that verified record. If the AI system is uncertain, it flags the gap rather than guessing.
The ‘Dr. Robbins’ Test
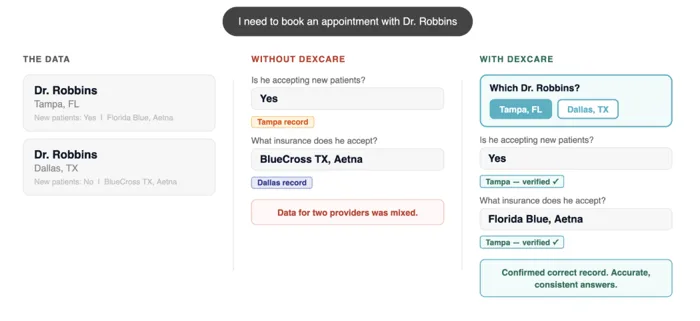
To see how the two types of AI and HITL models work, consider a large health system with two providers named Dr. Robbins. They share a last name, but one works in Dallas, the other in Tampa. They also accept different insurances.
A generative AI scheduling tool finds both but conflates the output, pulling “accepting new patients” from the Tampa record and “insurances accepted” from the Dallas record. The human approver, in this case a scheduler, may miss the error and book the visit. Nobody finds out until a patient arrives in Tampa and finds out that this Dr. Robbins won’t take their insurance. And nobody is happy.
On the other hand, a tool that uses AI to retrieve verified answers solves the problem. It uses the provider ID number to distinguish between the two Drs. Robbins. Then it locks onto a verified record and returns the same approved answer every time, matching the right Dr. Robbins to the right availability and insurance information every time. Schedulers at the end of this loop can book patient visits confidently, knowing that they’re choosing the doctor and location that best meets each patient’s needs.
What Specialty Scheduling Looks Like When the Data is Right
When AI is used to retrieve instant answers grounded in approved data, patient access teams can solve the many challenges associated with specialty scheduling. For example:
- A scheduler asks: “Patient wants a well-woman exam (WWE) for May 25, 2026. Her last WWE was July 21, 2025. Can I schedule?
- The AI says: “The requested data is only 308 days after her last exam. WWEs must be at least 366 days apart. The earliest she is eligible is July 22, 2026.” It then suggests a more appropriate visit type so the patient can still book an appointment.
- A scheduler asks: “I have a patient who wants to know if OBGYN does first-time telehealth consultations to see if they’re the right fit.”
- The AI says: “No. OBGYN does not offer first-time telehealth consultations for new patients.”
- A scheduler asks: “Patient wants a first-time cardiology visit.”
- The AI follows a decision tree, flagging the requirement for an EKG and referral before the patient can book, catching a potential wrong appointment before it happens.
In each instance, the human reviewer receives the accurate information they need to take the next step, whether it’s scheduling the appointment, finding a new visit type, or requesting required pre-appointment information. They also understand why the AI model made the recommendation.
Accuracy Is the Result
With Optimize AI from DexCare, health systems can build a single source of scheduling truth and put it to work across every channel a patient or scheduler touches. Optimize centralizes knowledge from documents, spreadsheets, and Visio charts in one place. When the system identifies a gap, it reaches out to the right subject matter expert, such as a scheduler or call center representative. Their answers get reviewed and added to the knowledge base automatically. Nothing goes live without human approval from an authorized member of your organization’s patient access team.
Optimize can read through a mountain of disconnected documents and existing files, and then surface gaps to human approvers. And, once human reviewers lock the data, 100% of information provided by the AI is grounded in verified, approved records.
Questions Worth Asking
The next time an AI vendor talks about their HITL capabilities, ask them these questions:
- Who approves the routing logic, and what does that approval process look like?
- What happens when a routing rule needs to change?
- Are AI outputs traceable and auditable? Can you show me the data source and which human approved the data before the AI used it?
If the answers to these questions are vague, HITL is a marketing phrase. If they are specific, then HITL is built into their architecture.
Humans—Not AI—Have the Final Say
Health systems that get reliable results from AI are those that make human approval an integral part of the process. Explore Optimize AI and see how a verified knowledge layer makes scheduling easy and reliable for patient access teams and the patients they serve.
The health systems that win tomorrow are the ones that get access right today. DexCare is the growth engine that gets them there.
- 40% more appointments, same clinical resources
- 5 fewer days waiting for care
- 25% increase in net-new patients