





Health systems have spent billions on scheduling tools. The infrastructure underneath them was never built to keep up.
Health systems have invested heavily in access and scheduling, and most still lose patients and leave capacity unused. Across the industry, spending on the tools meant to solve this—from scheduling platforms and digital front doors to call center modernization—totals $13.4 billion and growing. Yet the core infrastructure problem remains largely unsolved.
The infrastructure underneath patient navigation—the ability to match patients with available capacity the moment they look for care—was never designed for an environment where demand is growing, the supply of primary care physicians is shrinking, and margins remain under pressure. And the reason why starts with how scheduling logic works underneath the web directories, call centers, and countless booking features.
The Decision Tree Trap
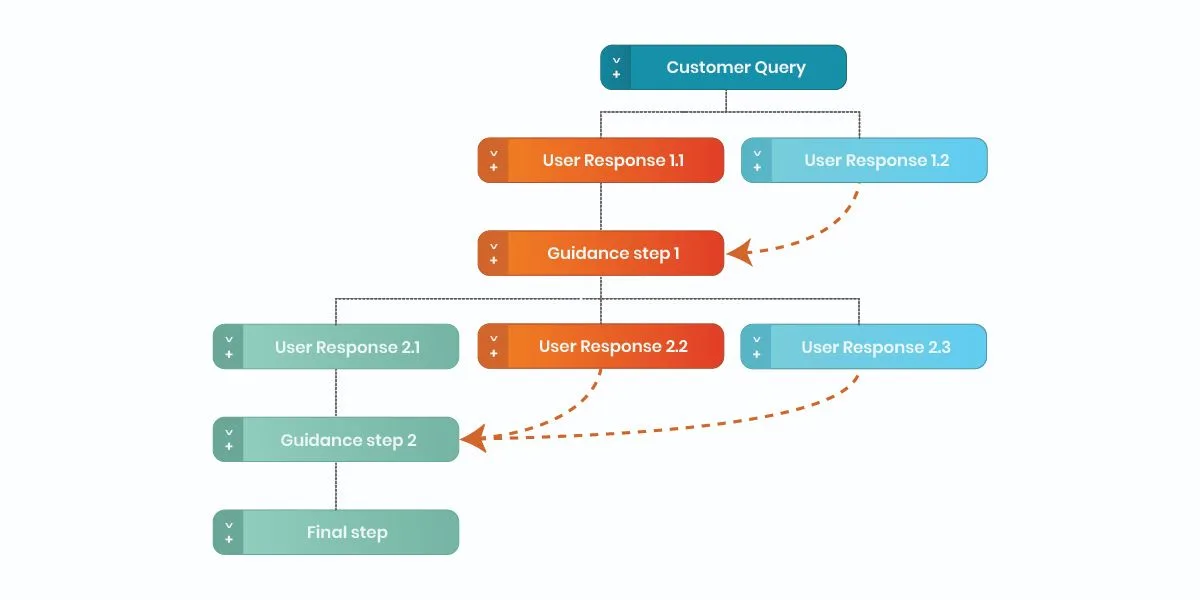
In theory, modern EMRs give health systems decision trees to route patients. In practice, those decision trees are static artifacts in a system that never stops changing.
One large, Florida-based health system has nearly 15,000 decision trees embedded in their EMR, each one reflecting years of accumulated clinical rules, operational constraints, and exception handling. That logic cannot be changed fast enough to reflect current priorities, capacity constraints, or care models.
What should be a strategic lever has turned into technical debt.
Specialty scheduling runs on decision trees built manually by cadence specialists, stored in Visio files and SharePoint folders, and outdated before they go live. Entire teams and external consultants are dedicated to a build-launch-redo cycle that never ends. Tribal knowledge lives in people’s head. When provider preferences change, workflows break. And when a service line activates, the queue starts over.
The Illusion of “We Already Do This”
Talk to any access or digital team and the same list of investments comes up: online scheduling, revamped websites, call center modernization, CRM journeys, SMS tools. On paper, it sounds like the patient navigation problem should be solved.
But look closely at how these initiatives work:
- Each channel implements its own copy of scheduling rules and provider data. When something changes in the network, every channel requires a separate update.
- Changes in network strategy or capacity require ticketing EMR analysts, updating PDFs, retraining staff, and hoping nothing falls through the cracks.
- “Navigation” becomes a human heroics problem with “super-users” who know which clinic stopped accepting a certain plan, which cardiologist sees athletes, or which MRI machine has been down all week.
The result? Patient navigation looks modern on the surface, but underneath it remains powered by spreadsheets, tribal knowledge, and static EMR configuration. The root cause is structural with no shared infrastructure governing how patients get matched to care.
The Control Plane for Patient Navigation
The answer? Not another app in front of the EMR, but a dedicated infrastructure layer—a navigation control plane—that sits between raw operational data and every channel where patients and staff interact.
That platform does four things no point solution does today:
- Maintains a single, continuously updated source of truth for provider, location, and insurance data, so every channel is working from the same reality, not its own outdated copy.
- Digitizes clinical and operational logic in a way that non-technical teams can update in hours, not quarters, without opening a ticket or calling a consultant.
- Orchestrates decisions across the EMR, CRM, contact center, and digital front door, so channels uses the same navigation logic, not its own ad-hoc rules.
- Makes every navigation decision visible, so leaders can see where patients drop off, where capacity sits unused, and which rules are driving outcomes.
When navigation is treated as infrastructure rather than a feature, the rules governing it become programmable. It’s updated once and applied everywhere, instantly.
Why Not Just Let AI Solve It?
Many organizations are racing to deploy AI agents for scheduling, triage, and intake. The temptation is to point a large language model at existing knowledge—your data—and call it intelligence.
That approach introduces three compounding risks:
- Faster bad decisions. If the underlying data and rules are wrong, AI will reach the wrong conclusion more quickly, more confidently, and at greater scale than any human ever could.
- Uncontrollable variability. Each AI use case develops its own implicit rules from different documents and prompts, making it nearly impossible to govern, audit, or override decisions consistently.
- Change fatigue at machine speed. Every time the network, template, or clinical guideline changes, prompts and reference content must be manually updated across dozens of agents, creating an entirely new class of maintenance burden.
The alternative is to fix the data and logic layer first, then layer AI on top of it. This is where the navigation control plane becomes the foundation.
Leading health systems are replacing manual decision tree maintenance with AI-powered workflow management systems that ingest institutional knowledge and structured data to identify gaps and make updates in real time. That capability lives inside the navigation control plane, not alongside it. Here, the platform governs the knowledge and data, and AI handles the interaction. And that separation is what makes AI in healthcare reliable.
Stop Thinking in Features. Think in Platforms.
For marketing, digital, and access leaders, the shift in perspective is subtle but consequential:
- The goal is not to launch another front-door experience, but to ensure every front door calls the same navigation brain.
- The question is not “How do we make online scheduling easier?” It is “What is the platform that governs every decision about where patients go and in what sequence?”
- Success is not only measured in clicks or completed appointments, but in reductions in leakage, time-to-care, unused capacity, and staff effort.
Patient navigation is the strategic control plane of the modern health system. Treating navigation like a feature inside individual point solutions underestimates both the complexity of the problem and the scale of the opportunity. The systems that recognize this will stop patching the problem and start solving it. And the ones that don’t will keep watching capacity go unused and patients finding care somewhere else.
By Rakshay Jain, chief product officer, DexCare


